
How do climate change and health interact in Kenya’s pastoral drylands?
/
February 2026
Jackson Wachira PhD1, Peter Hailey, OBE1, Matt Fortnam, PhD1,2, Anne Khisa, PhD1, Steven Squires, PhD2, Tinkle Chugh, PhD2 & Nancy Balfour1
Affiliations: 1Center for Humanitarian Change and 2University of Exeter
Pastoralist communities in Kenya’s drylands interact with events such as drought and floods, which are an integral part of their ecosystem. These pressures shape everyday life, but they can disrupt wellbeing and the health systems of pastoral communities. This is especially so in recent decades, when climate change has increased the frequency and intensity of these events.
In this blog, we highlight some of the emerging climate-related health risks and the strategies pastoral communities and actors employ in response. We also share some ideas for enhancing the capacity of pastoral health systems to respond to and manage climate-related disruptions and outline how the Health System Resilience to Climate Surges (HERCS), which is part of the CLARE program, is contributing to pastoral health systems that can maintain continuity of care even as climate change becomes more pronounced.
These reflections are based on recent field visits in Marsabit and Turkana, Kenyan ASAL counties that are at the forefront of climate change. In both counties, we held introductory consultative meetings with communities, county departments of Health, meteorological departments, NGOs, and community health promoters (CHPs) as part of the introductory phase of the HERCS project.

Pastoral communities are experiencing new climate-related health risks
Pastoral regions are increasingly exposed to novel and changing health risks associated with climate change. During our discussions at Turbi, a small village in Marsabit, for instance, women reported that malaria, once absent from the area, has become common. As one woman stated, ‘ the mosquitoes have increased, resulting in fever in children.’
This shift is striking given that malaria has traditionally been endemic in Kenya’s lake and coastal regions, not in drylands. Alarmingly, some analysts observe that the malaria-causing vector in the drylands is resistant to some insecticides, posing a concern for its control.

In Turkana, some of the health sector actors we spoke to pointed out that malaria morbidities in the region were increasingly becoming unresponsive to treatment, particularly in cross-border areas. Climate change is also reconfiguring pastoral communities’ experiences with diarrhoeal diseases, a compound risk that interlinks with malnutrition and can have lifelong consequences. Health workers observed that the dispensaries experience a surge in diarrhoea cases in February, which is the peak of the dry season. For them, the contamination of water sources (for instance, due to shortage and increased sharing with livestock) accounts for the high caseloads
According to community accounts, droughts are increasing in intensity and have become more unpredictable in the two counties, impacting community health. Coupled with other factors such as poor coverage of potable water and chronic vulnerability due to years of marginalisation and weak care practices, drought results in increased malnutrition and multiple morbidities.
Residents in both counties recalled that the severe Horn of Africa drought between 2020 and 2022 led to households losing up to 80% of their livestock – especially cows- which, when combined with existing malnutrition and changing health security, triggered widespread hunger and psychological distress. Malnutrition has enduring effects on the developmental, economic, social and medical well-being of individuals, communities and nations. These impacts are experienced by the affected generation but can run through generations.

Pastoral Communities (and actors) employ diverse strategies to mitigate climate-related health risks
In collaboration with various stakeholders, pastoral communities implement a wide array of strategies to address growing climate-related risks. Village-level dispensaries and health facilities run by county governments, and NGOs, work closely with Community Health Promoters (CHPs) to prevent, treat and refer ailments, including malnutrition. Cases that cannot be treated at this level are referred to higher levels of healthcare service delivery as outlined in the country’s current health policy. Health facilities are also useful points for public health education and for the prescription of essential health and nutrition products, including those in related domains such as water and sanitation (WASH).
Compared to other regions in Kenya, many pastoral settlements and communities are located far from health facilities, and communities often migrate further from settlements during drought. To reach these communities health and nutrition outreach programs organised by health departments, NGOs, and local health facilities play a critical role.
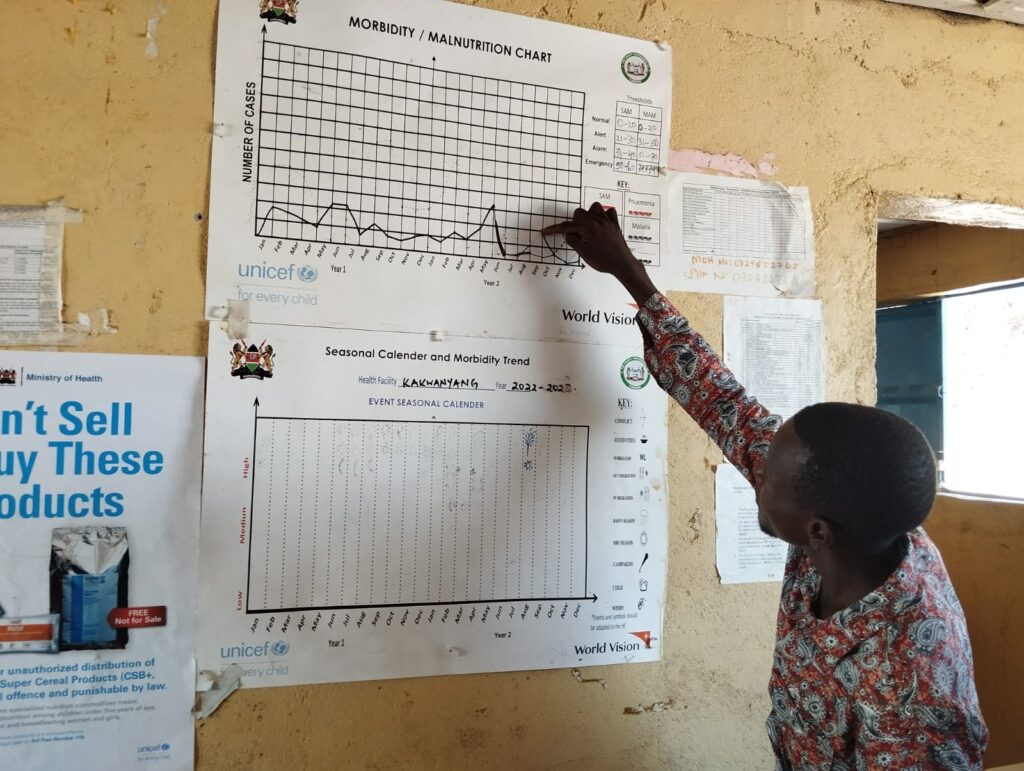
During outreaches, community health workers and facility health workers screen for health conditions and provide treatment for morbidities and malnutrition at villages, with complex cases referred to higher-level facilities. Outreaches also provide a space for health and nutrition workers to provide support and supervision to Community Health Promoters, who typically undertake similar tasks and follow-ups at their respective communities.
Health and Nutrition outreaches can be an integral part of the Surge Approach, an innovative model that enables health facilities to evaluate capacities and reorganise resources in response to shock-related surges in healthcare services. Over the years, the Surge Approach has been embedded in the day-to-day operations of the health system, complementing the existing community and health facility capacities. As we learnt, however, these activities have been greatly affected by decreasing external funding, especially the closure of several USAID -funded projects
While communities and health facilities can and do have established mechanisms to provide health and nutrition services, external support is crucial, particularly during extreme weather events when the demand for preventative, curative and restorative services exceeds the local capacity of the health system.
Pastoral communities also utilise informal, household and community-level practices to promote health and wellbeing. These include household and community-level care-giving, participation in loans and savings groups, and the sanctioning of state and non-state actors to respond to climate-related disruptions.
Research increasingly highlights the potential value of different facets of informal community health to bridge the wide health care access and utilisation gap, but also underscores the need for recognition and the establishment of structures that can promote the useful approaches, such as the use of ash when soap is unavailable, to prevent hygiene-related ailments, while limiting those that can result in adverse outcomes such as the use of certain herbs for treatment. In all, formal and informal health systems are typically interlinked, with Community Health Promoters playing a foundational role, but this interconnectedness needs more appreciation and strengthening.

Enhancing the Climate Resilience of Pastoral Health Systems
Climate change poses significant challenges to pastoral health systems. Demand for formal and informal preventative, treatment and referral health and nutrition services surges during extreme weather events at a time when the functioning of a health system may itself have been disrupted. Climate change is making these events more frequent and severe. Enhancing the resilience of the pastoral health system is therefore imperative to minimise climate risks.
Strengthening resilience of pastoral health systems requires leveraging existing practices and strategies employed by pastoral communities, recognising the significance and the overlaps between formal and informal approaches.
Through the HERCS, we are exploring how to better prepare health systems for climate-related surges in demand. Through our conversations and participatory activities with communities, health departments, meteorological services, NGOs, and Community Health Promoters, we’re learning about the specific challenges these communities face, and the existing capacities to reduce climate-change related disruptions.
Our next steps involve deepening our understanding of how climate patterns affect health service demand and working with communities to develop early warning and early action systems. We are also exploring how innovations like improved forecasting could be integrated into existing approaches like the Surge model.
The challenge is clear, but so is the path forward: supporting what communities are already doing well, filling the gaps, and building systems that can withstand the climate challenges ahead. Yet, enhancing health system resilience also requires addressing the underlying causes of vulnerability: investing in basic infrastructure like well-equipped health facilities, reliable roads, functional markets, clean water systems, and supporting accountable governance at all levels.
Categories
Countries
CLARE Pillars
CLARE Themes
CLARE Topics
Published
CLARE Projects
CLARE Partners